My most recent adventures have given me a taste of the way the government is run and how it spends. Last month I worked a number of weeks for the Federal Government as a Census Enumerator, a person who bravely knocks on doors of those who have not yet filled out their census form by mail or on-line. It struck me then, as it does now, as a monumentally wasteful project. I had a mind-boggling 499,999 co-workers across the country. Why so many? As of last month, 40% of households remained uncounted. 40%! And in some areas the number was much higher. To wit: I received a message recently for extra pay if I would go to Atlanta for a week or two to help that team. Travel, room and board all paid. THERE HAS TO BE A BETTER WAY! The last Census in 2010 cost you and I almost $13 Billion. This year’s, despite the introduction of online forms, will cost much more. Why do we do this? The government certainly has the data it needs. But federal law “protects” us and (ostensibly) does not allow sharing of

information across departments. The Census is run under the Department of Commerce and they are siloed. They cannot share data with the IRS, Social Security, or any other department that owns demographic data. And vice versa. Crazy stupid, and as a result, we will have a woefully undercounted Census that favors households with internet access and those that trust it. The Census has always used an extrapolation factor and won’t that be interesting when each community earns a different factor. It is a mess, and we pay BILLIONS for this antiquated process every decade. With the ubiquitous cell phone, it’s time to send texts to everyone with links to an online survey. Sure, the details would have to be ironed out, but even paying a stipend to each household for filling out the survey would save billions of dollars.
I also had a taste of work as a State government employee, as a COVID-19 Contact Tracer for the Indiana State Department of Health. Although, truth

be told, I have not been behaving all that well the last few months (pandemic-wise), I was really looking forward to helping to make a difference. Back in May, out of curiosity, I took an online Contact Tracer course sponsored by Johns Hopkins Medical Center. During that course I
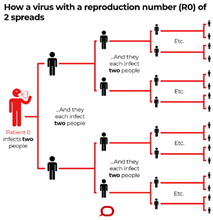
learned that the Reproductive Number (R0), or the number of people an average COVID-19 patient would infect, is between 2 and 3, about the same as the Influenza virus. For perspective, the R0 for Measles, a much more contagious virus, is 15. Still, if we can identify and isolate positive virus cases and quarantine their contacts, the spread of this virus will be reduced significantly.
I will tell you right here that this experience was very frustrating and wholly disappointing.
The Johns Hopkins course trained Tracers to call COVID-19-positive cases, inquire about symptoms in order to provide customized guidance on isolating, and identify people who may have been exposed to the virus during the contagious period (“Close Contacts”). The Tracers would then call the Close Contacts to encourage quarantining. The course also included training on interviewing skills since there was no specific script to the calls, only an outline of the major points. Fast forward to mid-September and the reality of the situation had changed, at least for the Indiana State Department of Health. It is understandable that not everyone is well-equipped to drive these interviews which can easily go off the rails. A script is probably necessary. And longer-tenure Tracers have told me that the initial script was workable. What is so very unfortunate is that over time the script has become so bloated that it is all but impossible for a patient to tolerate what has become a telephone intrusion lasting over an hour!

The Indiana State Department of Health (ISDH) has hired a company called Maximus to handle the Contact Tracing. Maximus also coordinates the Medicaid program in Indiana. Maximus executes the program at the direction of ISDH, which is solely responsible for the scripts. I can easily picture meetings at ISDH where each week someone has an idea that this or that demographic, or specific piece of medical information, would be helpful to include in the interview. And of course, the lawyers must weigh in and add interminable disclaimer paragraphs. The script expands each week and has now become unwieldy.
Consider a call to a positive COVID-19 case. First, there is a chance that we are letting the patient know for the first time that they tested positive. Fun. Then, of course, there is a good chance that the patient is feeling sick. We heard a training call where the patient, barely able to speak, had to excuse herself to vomit in the background. More fun. The calls start out with the positive test news and cruise into 6 demographic questions (sex, race, ethnicity, etc). Then we begin asking about symptoms and hospitalization. There are quite a few cases that are asymptomatic, and they say so, but the ISDH and the lawyers still require the Tracers to ask individually about some 20 different symptoms, including pneumonia. We then ask individually about 6 or 7 pre-existing conditions like COPD, kidney or lung disease. Hospitalization and testing questions come next, even for those who are feeling fine. Following that we are required to ask all, even babies and children (well, their guardians), if they are employed. And if they are, we capture full employment information in the database. FINALLY, after at least a half hour on the phone, we provide CDC guidance on isolation.

Symptomatic: Isolate for at least 10 days after symptoms started, when fever-free for 24 hours and there is improvement in all other symptoms
We ask questions about how feasible isolation will be and if the patient will require any support. Tracers are armed with contact information for an impressive list of resources such as food, medical care, housing, laundry, childcare, groceries, safety. We also provide directions on what to do if the patient suddenly becomes ill. We read two full paragraphs discussing what to look for and how to speak to a 911 operator or ER admission desk.
NOW, finally, we get to the Contact Tracing part of the call where we ask about people (and animals!) they have been in contact with. But rather than being open-ended, it is fully scripted, eg: Have you been to the grocery store? Have you been to school? The patient must wade through about 12 different questions regarding their whereabouts for the last few weeks. Trust me, it is painful. And of course, we capture the responses and request names, locations and phone numbers of each potential contact. The calls, when completed took well over an hour and were painful for the patient to tolerate. It’s clear that in an effort to collect helpful data, the calls have become unwieldy and have drifted from their original intent. They feel like an intrusion, not a service, and I did not enjoy it.
To make matters worse, it was very common for a patient to tell me, with some frustration, that they had already gone through a full Tracing phone interview. Many local health departments and/or school districts or Universities have installed their own Contact Tracers to more quickly isolate and quarantine. And of course, due to HIPAA laws, this information cannot be shared, even with the State Health Department.
In some ways, the calls to those who may have been exposed to a COVID-19 patient (Close Contacts) were worse. We would call a Close Contact and encourage them to quarantine for 14 days. We cannot tell them who the infected patient is, in fact we don’t even know. But the interesting thing is that about 50% of all calls in Indiana require an interpreter, the vast majority in Spanish. So we patch in an interpreter who becomes the go-between for me and the Contact. It’s clear that many Close Contacts are blue collar workers, like landscape workers or painters, who don’t get paid if they don’t work. Imagine being told that you must stay home for 2 weeks with no pay even though you feel fine. Many hang up the phone. And those that don’t are in for an extended 3-party telephone call.
During my second week, I strayed from the script. I paraphrased, combined symptoms, and skipped sections that were irrelevant. I shortened the guidance and the calls were much, much better. But I was warned that calls are scored and those that do not stick closely to the script are rated as failures and the Tracers are subject to disciplinary action and termination. I saved them the time and effort and sadly, quit after my second week. I am bummed about it, but I didn’t feel like I was helping. In fact, I thought I was bringing undue angst and emotion to people who were already nervous and vulnerable.
So, my government worker experience is now behind me and I got an up close and personal taste of government spending. As a Census worker I was paid $25 an hour with a bonus for weekend work. The hourly rate for a Contact Tracer is $30 with overtime always available at $45/hr. That’s over $60,000 annually; almost double what a new School Teacher is paid. Our government spends freely, and every single program adds tremendous obligations. The government passes out a mind-boggling amount of our money, and no matter your political persuasion, I’m confident you’ll agree that there needs to be better stewardship.
Be safe and sane, and as always, Thanks for reading.

No surprise here!! Years back there was a group called Liberty Amendment that figured out that if we could eliminate all the government businesses, we could then eliminate income taxes. I think that the government should head these pay out agencies with mothers of big families. I think we’d cut to bare bone spending. It couldn’t be worse! Thanks, Frank….
LikeLike
I see this effect REGULARLY with systems our clients have built at their own workplaces and we are tasked with fixing. Bloated and unhelpful services are everywhere – I don’t think it’s exclusive to gov’t programs. Silly about not being able to share information between gov’t services!!
LikeLike